
T1D Guide
T1D Strong News
Personal Stories
Resources
T1D Misdiagnosis
T1D Early Detection
Research/Clinical Trials
Leon Rock and the African American Diabetes Association: Continuing a Legacy of Black Health Advocacy
During Black History Month, the African American Diabetes Association (AADA) is drawing national attention as an African American-led organization confronting diabetes disparities in Black communities. Co-founder and CEO Leon Rock is advancing a hyperlocal, culturally grounded strategy designed not only to improve diabetes management but to dismantle the systemic barriers that have transformed a manageable condition into a generational health crisis.
.jpg)
.jpeg)
Through policy engagement, education and grassroots organizing, the organization is positioning itself as both a continuation of historic Black health movements and a modern force in diabetes advocacy.
A Public Launch Rooted In Urgency And History
The African American Diabetes Association publicly announced its formation during Black History Month in 2022. The timing was deliberate.
For years prior, Rock and fellow organizers had been studying diabetes data, examining hospitalization trends in the District of Columbia, Maryland and Virginia and meeting with faith leaders and community stakeholders. The work was already underway long before the announcement.
But the COVID pandemic accelerated the urgency.
Diabetes emerged as one of the strongest risk factors for severe COVID illness and death. Communities already experiencing high rates of diabetes saw disproportionate hospitalizations and complications.
“We had been working on this for years,” said Rock. “But we never said, ‘We are here.’ We never said, ‘We are born.’”
Black History Month became the moment to formally declare the organization’s presence.
For Rock, the announcement also carried historical meaning. In 1915, Booker T. Washington launched Negro Health Week to mobilize faith-based institutions and local leaders to address public health disparities in Black communities. That effort eventually expanded nationwide before the federal government discontinued it in 1951.
Rock views the African American Diabetes Association as a continuation of that organizing tradition.
“We are an extension of that movement,” he said. “Health is wealth.”
Understanding The Scope Of Diabetes Disparities
The work of the African American Diabetes Association is grounded in stark data.
Between 12% and 16% of Black adults have been diagnosed with diabetes, compared with about 7% of white adults. African Americans are 60% more likely to be diagnosed and nearly twice as likely to die from diabetes-related complications.
The disparity extends to outcomes.
Black patients are more than twice as likely to develop end-stage renal disease. They are significantly more likely to undergo lower limb amputations. Hospitalization rates for unmanaged glucose levels remain disproportionately high in predominantly Black communities.
“These numbers are not accidental,” Rock said. “They are systemic.”
Rock points to layered barriers that shape these disparities:
• Food deserts with limited access to fresh produce
• Pharmacy deserts where insulin and medications are difficult to obtain
• Health Professional Shortage Areas with limited primary care
• Insurance instability and generational poverty
• Historical medical mistrust

“These are structural realities,” Rock said. “They are not personal failures.”
The Three Fronts Of The Fight
Rock describes the fight against diabetes disparities as unfolding across three interconnected fronts: the DMV region, the Southern Diabetes Belt and the nation at large.
The DMV
The District of Columbia, Maryland and Virginia region serves as AADA’s home base. More than 500,000 residents in the region are impacted by diabetes.
In Washington, D.C., disparities are especially visible. Residents in predominantly African American neighborhoods experience significantly higher diabetes mortality rates than those in wealthier areas of the city. Black residents account for the majority of diabetes diagnoses in the District, reflecting longstanding inequities in access to preventive care, nutrition and consistent primary care.
“These are not random outcomes,” Rock said. “They are tied to access and investment.”
The Southern Diabetes Belt
The Diabetes Belt includes more than 600 counties across the Southern United States where prevalence reaches at least 11%. Mississippi, Alabama and Georgia are among the states most heavily affected.
The region is characterized by limited infrastructure for physical activity, underfunded healthcare systems and severe food deserts. Residents face a 30% higher risk linked to modifiable factors such as obesity. They also face a 37% higher risk tied to non-modifiable systemic factors such as poverty and limited healthcare access.
The Nation At Large
Across the country, disparities persist in urban and rural areas alike. Many communities are designated as Health Professional Shortage Areas, where consistent primary care access is limited.
Without early intervention and ongoing support, manageable conditions escalate into preventable complications.
Barriers Beyond The Diagnosis
When asked which barriers are impacting people most right now, Rock pointed first to accurate information.
Many individuals living with diabetes do not have consistent access to endocrinologists or primary care physicians (PCPs) trained in long-term diabetes management. Without reliable medical guidance, people are often left to navigate a complex condition on their own.
In that absence, misinformation can take hold.

Rock described the persistence of diabetes “folklore” within some communities — long-standing beliefs passed down through generations that oversimplify the disease. Diabetes is sometimes referred to casually as “the sugar,” a phrase that may sound familiar but can reduce a serious metabolic disorder to a single symptom.
“When you call it ‘the sugar,’” Rock explained, “you’re not capturing the full scope of what diabetes requires.”
Diabetes management extends far beyond elevated glucose levels. It involves cardiovascular health, kidney protection, nerve preservation, medication adherence, routine monitoring, preventive screenings and, in many cases, the use of technology. Without comprehensive education, the condition can be misunderstood as something far simpler than it is.
Continuity of care presents another significant challenge. Many individuals do not have a regular physician they trust or consistent access to specialists. Historical injustices and systemic inequities in healthcare have contributed to deep mistrust in medical institutions. That mistrust is rooted in documented history and lived experience.
Without trust, sustained engagement in care becomes difficult.
Structural barriers further complicate management.
Food deserts limit access to affordable and nutritious options. A food desert is a geographic area where residents have limited access to full-service grocery stores and fresh produce. Instead, convenience stores and fast food outlets dominate the landscape.
Pharmacy deserts operate similarly. In some neighborhoods, residents must travel long distances to reach a pharmacy that reliably stocks insulin, glucose monitors and other essential supplies.
Many predominantly Black communities are also located within Health Professional Shortage Areas, meaning there are too few primary care providers to meet demand. Primary care is often the first line of defense against preventable diabetes complications. When that access is inconsistent, diagnosis is delayed, and management becomes reactive rather than preventive.
Rock emphasized that diabetes disparities do not exist in isolation. They are connected to food access, housing stability, healthcare infrastructure and economic opportunity.
A Volunteer-Driven Organization
The AADA operates as a volunteer-driven organization.
Board members and leadership volunteers live with diabetes or support family members who do. The structure is intentional.
“Our board is built on lived experience,” Rock said.
That lived experience shapes the organization’s programming, advocacy priorities and communication style. Education is not delivered from a distance. It is shared from within the community.
The organization hosts educational webinars and special events focused on culturally responsive diabetes education and community support. These sessions address nutrition, prevention, daily management and practical tools for navigating life with diabetes.
The goal is empowerment, not blame.
“We cannot shame people into health,” Rock said. “We must educate with respect.”

The HAIR Model And Trusted Spaces
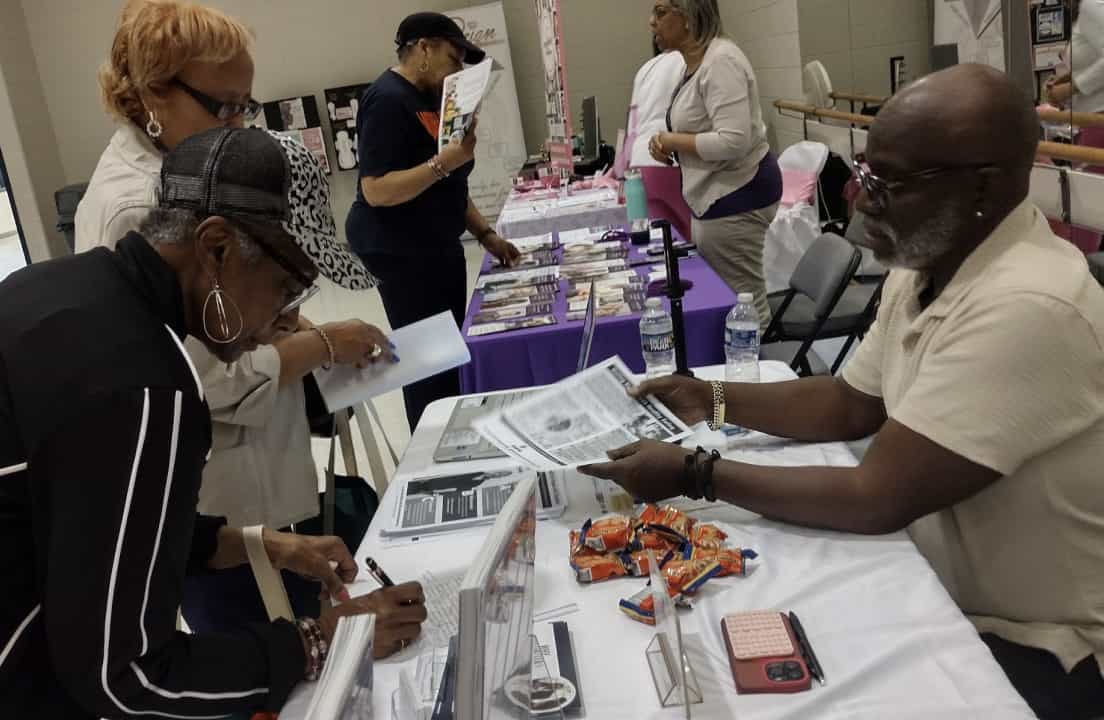
A central component of the African American Diabetes Association’s outreach strategy is its participation in the HAIR model, a Strategic Barbershop and Salon Partnership framework developed by Dr. Stephen B. Thomas.
Over the past three years, AADA has used this community engagement approach to deliver diabetes education, screenings and health information within barbershops and salons. These spaces have long served as trusted gathering places in Black communities, where conversations extend beyond haircuts to matters of family, politics and wellbeing.
Rather than requiring individuals to enter formal healthcare settings, the organization brings resources directly into environments where trust is already established. By doing so, it lowers barriers to engagement and encourages open dialogue about prevention, management and risk.
The strategy also complements partnerships with Historically Black Colleges and Universities (HBCU) and faith-based institutions. Churches with active health ministries provide additional venues for education and connection.
Rock believes that trusted cultural spaces can foster participation and sustained engagement in ways traditional clinical settings often cannot.
Trademark Tension And Institutional Resistance
The path to establishing the African American Diabetes Association was not without resistance.
During the trademark process, the organization encountered unexpected tension from a major national diabetes organization. The challenge surprised leadership, particularly given AADA’s focus on closing disparities and serving underserved communities.
Rock describes the experience as discouraging but clarifying.
The encounter reinforced the importance of independent leadership and community-centered advocacy. It also underscored the reality that systemic change can encounter institutional friction.
Despite the challenge, the organization successfully moved forward.

From Community Advocate To National Policy Voice
In October, Rock traveled to Capitol Hill alongside fellow advocates to discuss several diabetes-related bills under consideration. The visit marked an expansion of AADA’s advocacy from community education into federal engagement.
“If we are not at the table, our communities are not represented,” Rock said.
The conversation focused on legislation affecting people living with diabetes and policies shaping access to care. The appearance signaled that AADA intends to operate at both neighborhood and national levels.
Rock sees advocacy as a continuum. Education builds awareness. Community organizing builds power. Policy engagement builds scale.
Hyperlocal Chapters As A Future Vision
The AADA is developing hyperlocal chapter models across the country.
While the chapters are still emerging, the long-term vision is clear. Each chapter would operate within its specific community, addressing local barriers and leveraging local partnerships.
The hyperlocal model prioritizes:
• Hyperlocal chapters
• Faith-based partnerships
• HBCUs
• Barbershops and salons (HAIR model)
• Local advocacy
• Lived experience leadership
Rock believes sustainable change must grow from the pavement up.
Community Recognition And Local Validation
The organization has already begun receiving recognition at the local level. The Randallstown branch of the NAACP presented the African American Diabetes Association with its first community service award for its work educating Randallstown, Maryland, residents about diabetes awareness and prevention.

For a volunteer-driven organization, that recognition carried particular weight.
Because AADA’s strategy centers on neighborhood-level engagement, validation from a local NAACP chapter underscored that the work is resonating where it matters most — within the community itself.
Resilience Within The Black Diabetes Community
Despite the data and disparities, Rock speaks often about resilience within the African American diabetes community.
He described one board member in particular whose commitment continues to inspire him. She lives with type 1 diabetes and manages complications related to the disease. Even while navigating the physical and emotional demands of long-term diabetes, she continues to volunteer and serve as an active board member of the African American Diabetes Association.
Her work is not symbolic. It is practical and ongoing. She participates in planning meetings, community outreach and educational efforts, all while managing her own care.
For Rock, her presence represents something larger than individual perseverance.
“It shows what strength looks like,” he said.
He also points to caregivers who manage their own health while supporting parents or relatives with diabetes complications. That resilience, Rock said, is often overshadowed by statistics.
The narrative of disparity is real and urgent. But so is the story of individuals who continue to show up, volunteer and build support systems within their own communities.
“There is strength here,” Rock said.
For Rock, that strength is not accidental. It is generational. It reflects a long tradition of community care, mutual aid and collective responsibility within Black communities.

A Message To Those Who Feel Unseen
When asked what he would say to someone reading this article who feels unseen or exhausted by managing diabetes, Rock returns to community.
Start locally, he advises.
Look to community health centers. Contact your county health department. Explore your city’s department of health. Each state maintains a diabetes action plan.
Support may also exist through hospital-based diabetes education programs, church health ministries or local food banks that provide healthier options.
“You are your own best advocate,” Rock said.
Advocacy, he explains, begins at the local level. If resources are lacking, engage city and county representatives. Let policymakers know what is missing.
“All politics is local,” Rock said. “And diabetes care is local.”
A Continuing Legacy Of Black Health Advocacy
Rock holds a Master of Education from Cambridge College and an undergraduate degree from the University of Massachusetts College of Public and Community Service. He is months away from earning his PhD, formalizing decades of organizing with academic scholarship.
He also hosts The African American Diabetes Podcast, expanding education through dialogue and storytelling.
For Rock, the African American Diabetes Association represents both continuity and evolution. It honors the legacy of Negro Health Week while confronting modern diabetes disparities with data, policy engagement and culturally grounded outreach.
Black History Month highlights the African American Diabetes Association within a long tradition of Black-led health advocacy. But the organization’s mission extends far beyond February. Its work is year-round, rooted in sustained community engagement and long-term structural change.
The African American Diabetes Association has transitioned its monthly newsletter to Substack to build a more interactive, accessible, and powerful community. There you can find life-saving information, cultural health tips, and direct support straight to your inbox every month. All is welcome to join this new platform and stay connected to the heartbeat of Black diabetes health and wellness.
“We are here,” Rock said. “And we are building something that will last.”




.webp)





.webp)





.jpg)











.jpg)






%20(1).jpg)





.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)

.jpg)

.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)

.jpg)
.jpg)
.jpg)
.jpg)

.jpg)
.jpg)

.jpg)

.jpg)
.jpg)
.jpg)
.jpg)

.jpg)
.jpg)



.jpg)
.jpg)
.jpg)


.jpg)

.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)

.jpg)

.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)

.jpg)
.jpg)

.jpg)
.jpg)
.jpg)








.webp)