
T1D Guide
T1D Strong News
Personal Stories
Resources
T1D Misdiagnosis
T1D Early Detection
Research/Clinical Trials
Saliva, Not Needles: How T1D Scout Wants to Change Type 1 Diabetes Screening
When Yuta Matsuda was a child in Japan, dinner table conversations were often about patients. His mother, an endocrinologist, treated people living with type 1 diabetes (T1D). He grew up hearing about the fear, the late diagnoses, and the emergencies that might have been avoided if the risk had been spotted earlier.
%20(1).jpg)

Years later, as a geneticist and now CEO of T1D Scout, Yuta is trying to solve the problem behind those stories: most families at risk of type 1 diabetes are never screened in time.
Recently, he was invited to present his team’s work on The Sugar Science, where he shared a bold yet simple idea: replace clinic‑based, needle‑heavy screening with a saliva‑based genetic test that families can complete entirely at home.
This article is based on that intervention and walks through the core message: if we want to prevent the most devastating type 1 diagnoses, we need screening that is truly accessible to real families, wherever they live.
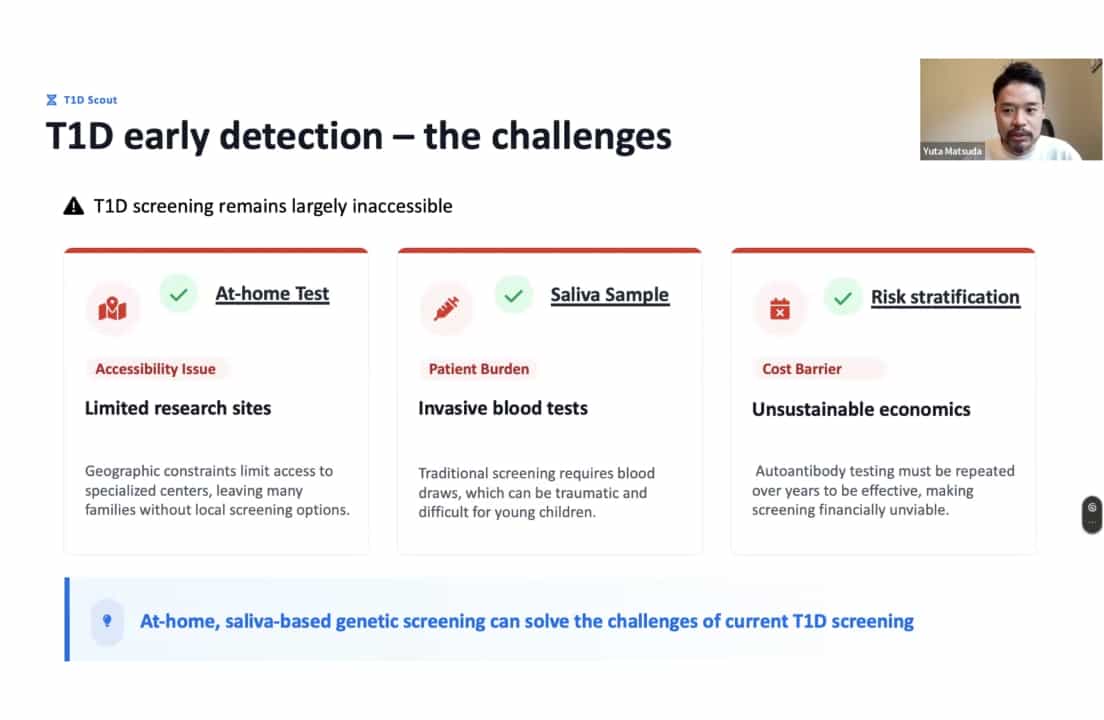
Why Current Screening Doesn’t Reach Most Families
On paper, we know what should happen. Medical guidelines recommend screening family members of people with T1D, especially children. In reality, only a tiny fraction of those family members are ever tested.
The reasons are not mysterious: Yuta and his team have interviewed nearly 100 families affected by type one diabetes and heard the same obstacles again and again. Access is the first problem. Screening programs are often tied to a handful of specialized centers. If you live far away, don’t drive, or can’t take time off work, getting to those centers regularly is nearly impossible.
The second problem is emotional. Traditional screening relies on blood draws, sometimes repeated over many years. Parents may be fully convinced that screening is important, but asking a four‑year‑old or a seven‑year‑old to face needles again and again is a huge psychological barrier.
“The awareness is there. The willingness is there. But the barrier stops them from moving forward,” said Yuta.
The third problem is sustainability. Running frequent blood‑based autoantibody tests in large groups is expensive and resource‑intensive. For general population screening, it simply doesn’t scale.
Put together, these issues mean that countless children at elevated risk are never identified early—even in families who want screening and actively worry about T1D.
T1D Scout’s Idea: Start with Saliva and Genetics At Home
T1D Scout’s proposal sounds almost too simple: move the first screening step into the home and use saliva instead of needles.
Families can easily participate in the study from home. Parents start by visiting the T1D Scout website where they find clear information about the project, give electronic consent, and answer a few questions about their child’s age and family history, such as whether any relatives have type 1 diabetes.
Once enrolled, a saliva collection kit arrives by mail. The child provides a small saliva sample at home—no needles, no hospital visits, no waiting rooms. The family then mails the kit back to a central laboratory.
In the lab, DNA is extracted from saliva and analyzed using a standard genetic test. Rather than looking for a single “diabetes gene,” scientists combine information from many different genetic variants to calculate a Genetic Risk Score (GRS).
This score provides a way to estimate a child’s risk of developing T1D compared with the average risk in the general population. It doesn’t diagnose diabetes—it simply indicates whether the child’s risk is higher, lower, or about the same as that of most children.
Children whose GRS shows a higher risk are offered closer follow-up.

This includes autoantibody testing via a small finger prick at home, avoiding repeated hospital blood draws. By using the GRS, researchers can identify children who may benefit from extra monitoring while keeping the process safe, simple, and comfortable for families.
In this design, genetic testing is the first filter. Instead of doing frequent autoantibody tests on everyone, T1DScout uses the GRS to focus attention and resources on the children most likely to benefit from intensive follow‑up. That’s what makes the model potentially scalable, both logistically and financially.
A GRS Built to Work in the Real World, Not Just in Studies
As Yuta explained during his talk at The Sugar Science, T1D genetic risk scores have existed for years. However, he made a crucial distinction: “Most of those models were designed for research, not for families.”
Traditional models often depend on imputation, a statistical method that “fills in” genetic variants that were not directly measured. While useful in research, imputation can introduce ancestry‑related bias and complicate regulatory approval. To date, no imputation‑based genetic test has been approved by the FDA.
T1D Scout’s Genetic Risk Score was built in a special way. It only uses genetic variants that are directly measured on a common DNA test—there’s no guesswork or “imputation” involved. The test uses DNA collected from saliva, with an FDA-approved kit and lab procedure, so it’s simple and safe to do at home.
The GRS was developed by studying several hundred children and adults with type 1 diabetes and healthy controls, and then validated against independent cohorts as well as more than 50,000 healthy volunteers from the UK Biobank to ensure it yields reliable results.
The result is very strong: the test can accurately tell which children are at higher risk of type 1 diabetes most of the time—about 90 out of 100 cases. This puts it on par with the best genetic risk models available today.
However, as Yuta points out, it’s not just about numbers on a chart. What really matters is that this test can actually be used in a real-life program, safely and easily, for children across the country, all from the comfort of home.
What Happened When More than 3,000 Families Signed Up
The real test is not in the code or the manuscript, but in what happens when real families use the system.
T1D Scout’s pilot program is fully remote, targets children under 19 with at least one T1D‑affected family member, and is approved by an institutional review board (IRB) with electronic consent.
The early results are impressive. Within a short time, over 3,000 families signed up for the study, more than 1,000 children received saliva collection kits, and over 800 samples were returned to the lab. That’s a return rate of more than 85%, which is unusually high for any at-home study.

Most participants are Caucasian, reflecting the current U.S. population affected by type 1 diabetes; the average age is 8, and almost all children have a confirmed family history, often involving a parent, sibling, or close relative.
When the Genetic Risk Score was tested in real-world settings, it performed as expected. Children identified as high risk were more than ten times more likely to test positive for multiple autoantibodies, a key sign of ongoing autoimmune activity.
Children in the low-risk group had rates of autoantibody positivity similar to what is seen in the general population, even though all of them had a family history of type 1 diabetes. In other words, even within a group already considered “high risk” by traditional standards, the GRS can distinguish which children are truly at elevated risk and which are closer to the average baseline.
Anxiety, Reassurance, and the Role of Counseling
One of the most powerful parts of Yuta’s talk at The Sugar Science wasn’t a chart—it was hearing how families feel when they get their child’s genetic test results. After a low-risk result, parents felt much less worried. For many, the test gave T1D families real peace of mind and helped them see the risk more clearly.
After a high-risk result, parents were initially worried, which is normal. But T1D Scout doesn’t just give a number. Families can talk to genetic counselors online and get emotional support, and after that, their anxiety usually goes down.
The most important point is that more than 75% of families had never been tested for type 1 diabetes before. This shows the program is reaching the people who need it most—those who knew there was a risk but didn’t have an easy way to get tested.
The Road Ahead: More Data, More Diversity, More Reach
During the Q&A at The Sugar Science, people asked whether the test works for families of non-European backgrounds. Because the new method uses only directly measured genetic data, it performs better than older tests for Latino and African-ancestry families, though it remains most accurate for people of European descent.

Yuta explained that’s why T1D Scout is running projects in Japan to adapt the test for East Asian populations and working with Latino communities to improve it for them.
The next big step is a clinical trial. It will compare starting with the genetic test and following up only with children at higher risk, to the traditional method of doing standard autoantibody tests for everyone.
The goal is to see which approach finds more children showing early signs of type 1 diabetes. The hope is that using the genetic test first will reach more families and catch T1D earlier in a simpler, more efficient way.
A Different Kind of T1D Story
At the end of his appearance on The Sugar Science, Yuta returned to where his story began: his mother’s clinic in Japan, and the children who arrived already in crisis.
T1D Scout’s work does not promise to prevent every case of type 1 diabetes. But it does point to a very different future: one in which a parent, worried because T1D runs in the family, can order a kit, collect some saliva at the kitchen table, send it off, and receive a clear explanation of their child’s risk—along with support and a plan for what comes next.
If this model continues to prove itself in trials and expands fairly across all populations, it could help rewrite thousands of T1D narratives.
Instead of “We found out in the ICU,” more families might someday say, “We knew early, we had time to prepare, and we weren’t alone.”
That is the vision at the heart of T1D Scout’s intervention: make early T1D risk screening simple enough, gentle enough, and accessible enough that no willing family is left behind.




.webp)

.webp)

.jpeg)






.jpg)













.jpg)












.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)

.jpg)
.jpg)

.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)

.jpg)
.jpg)
.jpg)
.jpg)

.jpg)
.jpg)

.jpg)

.jpg)
.jpg)
.jpg)
.jpg)

.jpg)
.jpg)



.jpg)
.jpg)
.jpg)


.jpg)

.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)

.jpg)

.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)








.webp)